
✨ ⚠️ Mpox Outbreak Resurgence: The Scientific Truths We Need to Know
With the World Health Organization (WHO) once again declaring Mpox a “Public Health Emergency of International Concern” (PHEIC) in August 2024, this virus has returned to the public spotlight. Understanding its evolutionary characteristics and scientific prevention knowledge is crucial for reducing the risk of infection.
🩺 Quick Summary
- Viral Mutation: The new strain, Clade Ib, is more infectious and pathogenic. The infected population has expanded from specific groups to the general public, including children.
- Transmission Routes: Not limited to sexual contact; close household contact, caregiving contact, and contact with contaminated materials can all lead to transmission.
- Scientific Response: Vaccination (MVA-BN) is a key preventive measure. Anyone experiencing fever accompanied by a rash should seek medical attention promptly for PCR testing.
📌 What is New About This Outbreak?
The core change in this outbreak is the emergence of the Clade Ib strain. Compared to the previously prevalent Clade IIb, Clade Ib has demonstrated higher transmission efficiency and pathogenic potential in the Democratic Republic of the Congo and surrounding countries [Source: WHO].
Prevention and control strategies have adjusted accordingly: while Mpox was previously thought to spread primarily among specific high-risk groups, current monitoring data indicates that the virus has spread through household contact and caregiving. The proportion of children among the infected population has increased. This means the focus of prevention has shifted from targeting specific populations to monitoring and prevention across the entire society [Source: WHO].
🧬 What Does This Mean for the General Public?
🔹 1. Identifying Typical Symptoms
The course of Mpox is typically divided into two stages:
* Prodromal Phase: Characterized by fever, severe headache, lymphadenopathy (swollen lymph nodes), muscle aches, and fatigue.
* Eruptive Phase: The rash usually progresses through the stages of maculopapular $\rightarrow$ vesicle $\rightarrow$ pustule $\rightarrow$ crust $\rightarrow$ desquamation (peeling).
* Special Note: Clinical manifestations of the Clade Ib strain may be more severe, with a wider distribution of rashes and faster disease progression [Source: Research Report].
🔹 2. Transmission Routes and Risk Management
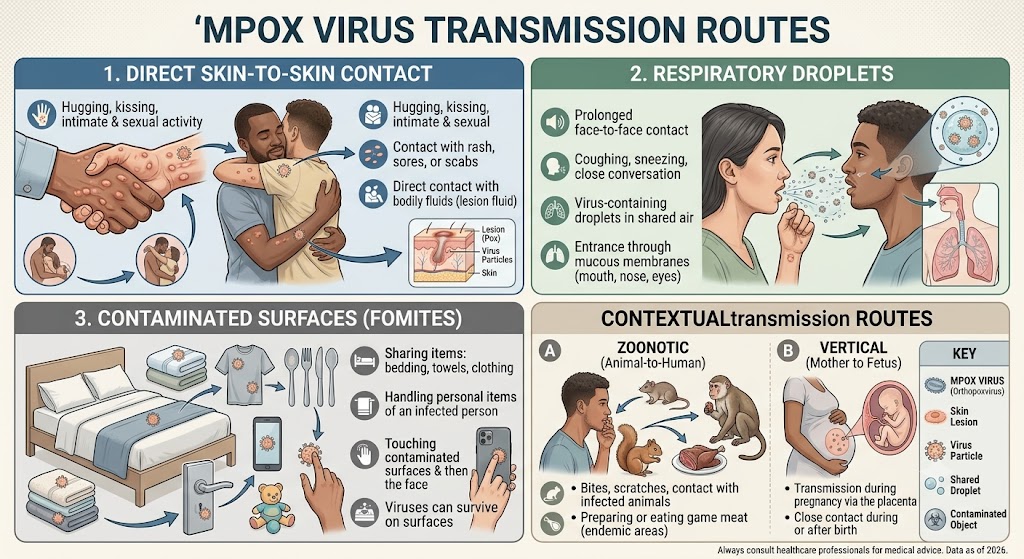
Mpox is primarily transmitted through the following ways:
* Direct Contact: Contact with an infected person’s body fluids, rashes, or contaminated items (such as bed linens and clothing).
* Vertical Transmission: Pregnant women may transmit the virus to the fetus.
* Medical Protection: In healthcare facilities, medical staff must take strict protective measures (such as wearing N95 masks and protective clothing). Those isolating at home must remain in isolation until all rashes have completely scabbed over and fallen off [Source: Research Report].
🔹 3. Vaccines and Prevention
The third-generation modified vaccinia vaccine (MVA-BN, such as Jynneos/Imvanex) is currently recommended. Vaccination strategies include prophylactic vaccination and post-exposure prophylaxis (PEP), the latter of which is recommended within 4 days after contact for optimal protection. If suspected symptoms appear, a PCR nucleic acid test should be performed immediately for confirmation [Source: Research Report].
💊 Points of Caution
There are still some scientific “knowledge gaps” regarding Mpox that require further research to clarify:
* Long-term Effects: There is currently a lack of systematic data on long-term sequelae (such as scarring or vision impairment) following Clade Ib infection.
* Vaccine Efficacy: More clinical evidence is needed to support the precise protection rate of vaccines designed for Clade II against Clade Ib.
* Treatment Protocols: The optimal clinical treatment regimen using antiviral drugs (such as Tecovirimat) for Clade Ib is still being explored.
* Asymptomatic Transmission: It is currently unclear whether Clade Ib has a significant asymptomatic transmission period [Source: Research Report].
🔬 Clarifying Common Misconceptions
- Misconception 1: Mpox is a “exclusive disease” of specific groups. Fact: Any population is at risk of infection after contact with the virus.
- Misconception 2: Mpox can be transmitted through food. Fact: Mpox is not related to food (such as bananas or other fruits); please do not believe rumors.
- Misconception 3: Antibiotics can treat Mpox. Fact: Mpox is a viral infection; antibiotics are ineffective against viruses. Do not self-medicate.
- Misconception 4: Mpox is the same as smallpox. Fact: Although both belong to the Poxviridae family, they are different viruses with different biological characteristics.
✨ Sources Used for This Article
- WHO. Mpox (monkeypox) outbreak 2024. 2024. URL: https://www.who.int/news-room/fact-sheets/detail/mpox
- Research Report. Global Mpox Epidemiological and Clinical Characteristics. 2024. (URL not provided in source material)
⚠️ Disclaimer: This article is for general health education only and should not be used as a basis for medical diagnosis. Please consult a qualified healthcare professional for medical advice.
© 慧子国際医療支援株式会社 All rights reserved | Unauthorized reproduction is prohibited.